INNOVATIVE SOLUTIONS FOR FORWARD AND WIDE DEPLOYMENT OF FLUORESCENCE-GUIDED DEBRIDEMENT
Our Mission
TO INCREASE THE EFFECTIVENESS OF DEBRIDEMENT PERFORMED BY INEXPERIENCED SURGEONS WHEN REPAIRING OPEN FRACTURE
To repair an open fracture, orthopaedic surgeons will peform open reduction internal fixation (ORIF) —a surgical procedure to align the bones and stabilize them with special hardware like plates, screws and rods.
About 150,000 ORIF procedures are performed on patients with open fractures in the US each year. A critical step in this procedure is a thorough debridement—the term used to describe removal of dead and devitalized tissue that is prone to infection and prevents proper healing. Proper debridement is crucial for preventing infection, which is a devastating complication of open fracture.
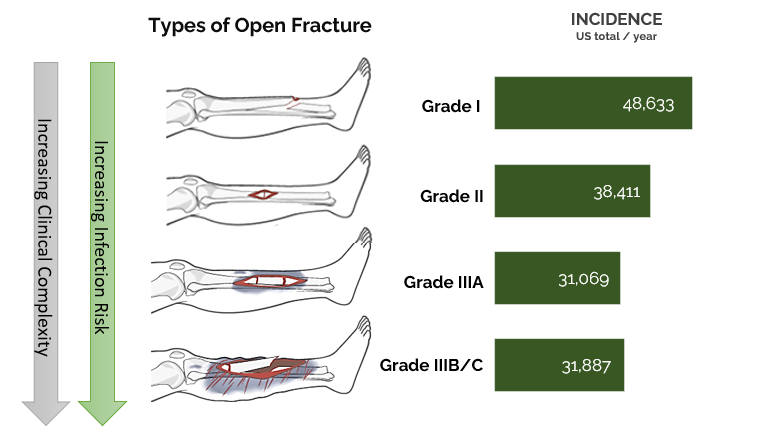
Nevertheless, about 5-30% of these fractures become infected after ORIF surgery, with high-energy open fractures (Gustilo Grade IIIA-C) being more succeptible to deep surgical site infection. Half of these readmitted patients will undergo a series of repeated surgeries and antibiotic treatments in an effort to manage the chronic infection. Long term disability, poor quality of life and often, conversion to amputation is the outcome for these patients.
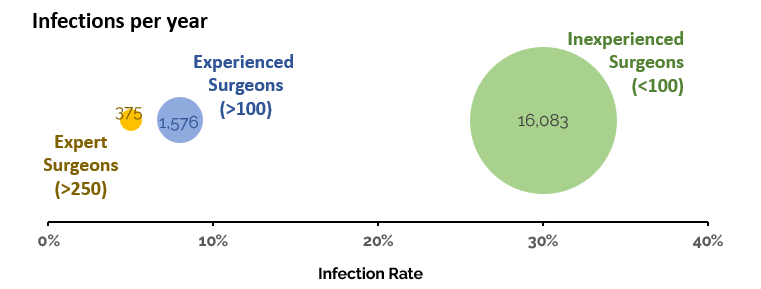
There is a huge variation in outcomes between more and less experienced surgeons, resulting in an excess of readmissions.
Trauma can occur anywhere, and specialists are not always accessible. Half of ORIFs are performed by less-experienced surgeons, often at smaller hospitals without access to the most state-of-the-art imaging and intraoperative near-infrared fluorescence equipment. Even at larger hospitals and designated trauma centers, patient complexity isn't always matched perfectly to practicioner skill, and new surgeons must gain experience through practice.
The patients of surgeons who perform more than 250 ORIF surgeries each year have about a 5% rate of infection, compared with the patients of inexperienced surgeons (less than 100 ORIFs per year), who have an infection rate of 30% or more.
This variation in care is unacceptable and unnecessary with advanced fluorescence guided surgery technology. FWD Imaging Inc. aims to develop hardware and analytic software to provide all surgeons with enhanced guidance during this critical procedure. In doing so, we hope to eliminate the burden of unnecessary infections that occur in tens of thousands of patients each year and cost our healthcare system 1.2 billion dollars annually.
Our Technology
TECHNOLOGY ENGINEERED FROM DECADES OF SCIENTIFIC RESEARCH AND CLINICAL EXPERIENCE
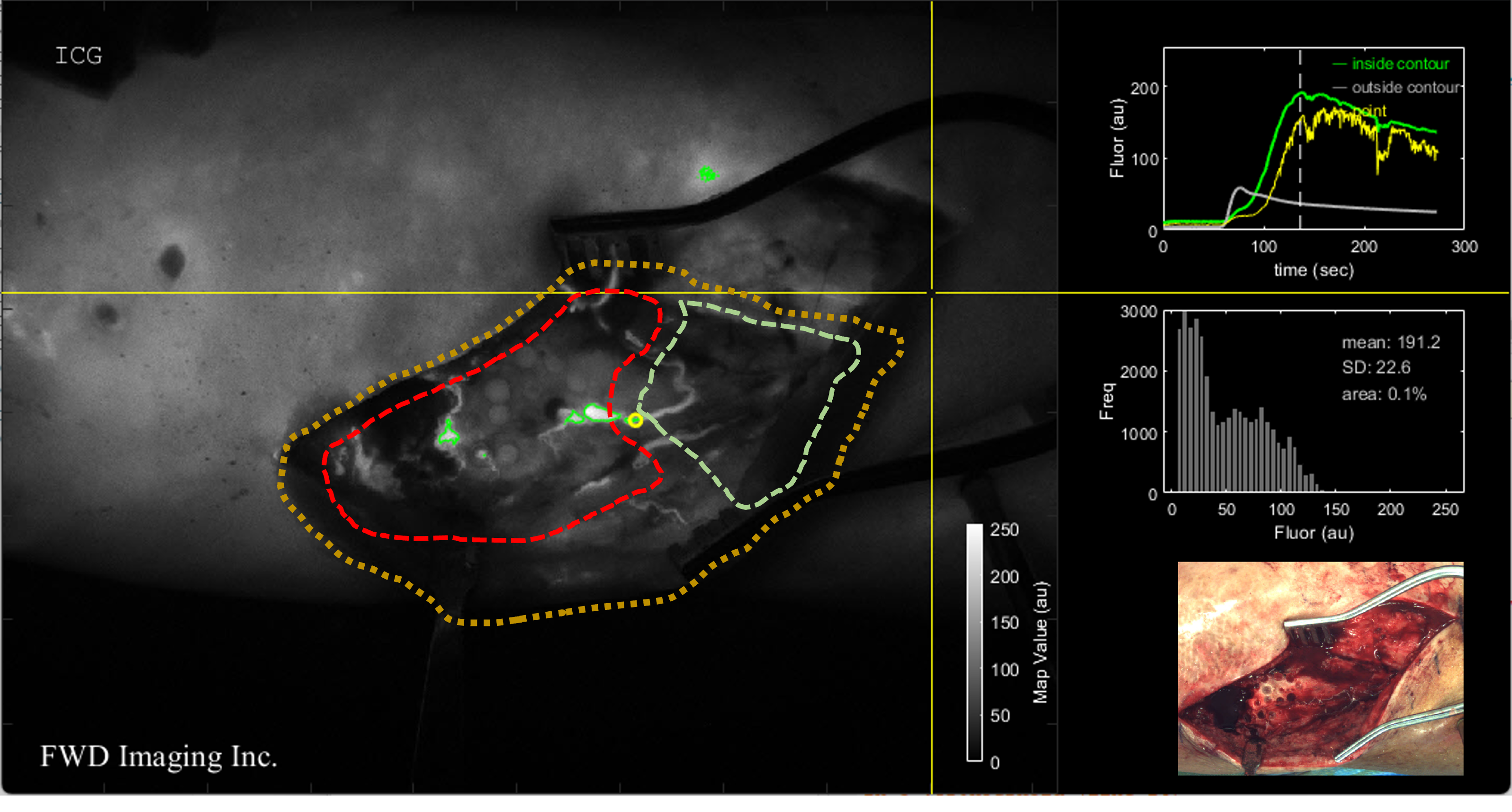
State-of-the-Art Fluorescence Guided Surgery—using FWD Imaging Inc's proprietary quantification methods and superior hardware—can provide surgeons with live intraoperative assessment of tissue viability.
Our publications and intellectual property below provide publically-disclosed details of our unique approach to managing patient variability and producing quantitative information. If you'd like to further discuss our technology within the context of an NDA, please email us using the addres below.
Surgeon's live view showing "risk contours"
The Team
We are an early-stage biotechnology start-up co-founded by faculty, students, and engineers from Dartmouth Health and Dartmouth College in Hanover, New Hampshire. Our multidisciplinary team is advancing innovative hardware solutions for fluorescence-guided surgery leveraging a rapidly growing field intraoperative guidance.
I. Leah Gitajn, MD, MHCDS
Co-Founder and President
Jonathan Thomas Elliott, PhD
Co-Founder and Treasurer
Petr Bruza, PhD
Co-Founder and Secretary
Shudong Jiang, PhD
Co-Founder
Jeffrey Renk, BSEE
Co-Founder
Yue Tang, BE, PhD Candidate
Co-Founder
J. Scott Sottosanti, AB/BE
Co-Founder
Publications and Intellectual Property
Elliott JT, Gitajn IL, Jiang S, Pogue B. Method and apparatus to measure bone hemodynamics and discriminate healthy from diseased bone, and open reduction internal fixation implant with integrated optical sensors. United States patent application US 17/290,991. 2022 Mar 31.
Elliott JT, Addante RR, Slobogean GP, Jiang S, Henderson ER, Pogue BW, Gitajn IL. Intraoperative fluorescence perfusion assessment should be corrected by a measured subject-specific arterial input function. Journal of biomedical optics. 2020 Jun 1;25(6):066002. doi: 10.1117/1.JBO.25.6.066002
Han X, Demidov V, Vaze VS, Jiang S, Gitajn IL, Elliott JT. Spatial and temporal patterns in dynamic-contrast enhanced intraoperative fluorescence imaging enable classification of bone perfusion in patients undergoing leg amputation. Biomedical Optics Express. 2022 Jun 1;13(6):3171-86. doi: 10.1364/BOE.459497
Gitajn IL, Elliott JT, Gunn JR, Ruiz AJ, Henderson ER, Pogue BW, Jiang S. Evaluation of bone perfusion during open orthopedic surgery using quantitative dynamic contrast-enhanced fluorescence imaging. Biomedical Optics Express. 2020 Nov 1;11(11):6458-69. doi: 10.1364/BOE.399587
Elliott JT, Jiang S, Pogue BW, Gitajn IL. Bone‐specific kinetic model to quantify periosteal and endosteal blood flow using indocyanine green in fluorescence guided orthopedic surgery. Journal of biophotonics. 2019 Aug;12(8):e201800427. doi: 10.1002/jbio.201800427
We are currently seeking early stage seed funding, and would invite angel investors and VCs to contact us to discuss opportunities to support our mission.
Developing solutions to guide orthopaedic trauma to enhance the performance of inexperienced surgeons.